ERM & Macular Hole: Surgical Decision Points
Epiretinal membranes and macular holes. Staging, progression indicators, and when to refer for surgical consultation.
ERM & Macular Hole: Surgical Decision Points
Epiretinal membranes and macular holes are the two most surgically significant vitreomacular interface disorders in primary eye care. OCT is indispensable for both — it provides the exact staging information retinal surgeons need before PPV, and helps you identify which patients need urgent referral vs. safe monitoring.
Epiretinal Membrane: OCT Staging
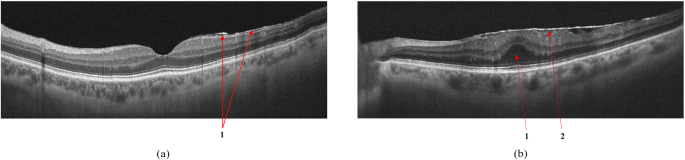
The Govetto et al. staging system (2017) provides an OCT-based ERM classification with surgical implications:
| Stage | OCT FeaturesVisual Impact | Action | |
|---|---|---|---|
| Stage 1 | Thin hyperreflective layer on ILM; foveal depression preserved; EZ intact | Minimal symptoms | Monitor annually |
| Stage 2 | Thicker membrane; foveal depression blunted; all layers identifiable | Mild metamorphopsia, VA usually preserved | Monitor 6 months |
| Stage 3 | Foveal contour abnormal; EZ disrupted; some layers indistinct | Moderate VA loss, significant metamorphopsia | Consider referral |
| Stage 4 | Severe foveal distortion; EZ absent subfoveal; ectopic foveal architecture | Significant VA loss | Refer for surgery |
ERM: Key OCT Measurements
- Central macular thickness (CMT): Increased in most ERMs; >320 μm suggests significant traction. But CMT alone doesn't determine surgical need.
- EZ band continuity: Single most important predictor of post-surgical visual acuity. Continuous EZ → good prognosis. Disrupted EZ → guarded prognosis even after successful membrane peeling.
- Inner retinal layer architecture: Can you still identify GCL, IPL, INL as distinct layers? Preservation correlates with better outcomes.
- Foveal avascular zone (FAZ) on en face: ERM traction can distort the FAZ — visible on ILM en face as irregular central reflectivity pattern.
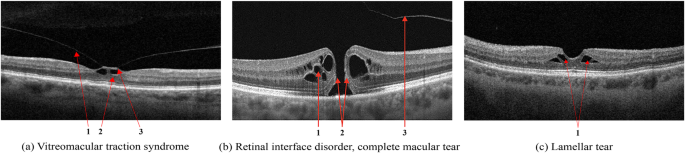
Vitreomacular Traction (VMT)
VMT is an incomplete posterior vitreous detachment where the posterior hyaloid remains adherent to the fovea while detaching elsewhere. On B-scan:
- The posterior hyaloid appears as a hyperreflective line elevated from the retinal surface
- It remains attached at the fovea — causing a "tent" or "peak" elevation of the inner retinal surface
- Cystoid spaces in the fovea are common (pseudo-hole morphology on clinical exam)
- VMT footprint width: <1500 μm = focal VMT; often resolves spontaneously or with ocriplasmin
- VMT footprint width: >1500 μm = broad VMT; higher likelihood of spontaneous VMA, lower ocriplasmin response
Macular Hole: OCT Classification
The IVTS classification (International Vitreomacular Traction Study) uses OCT measurements to stage macular holes:
| Stage | Minimum Diameter | Surgical Urgency | Expected Closure Rate |
|---|---|---|---|
| Small | <250 μm | Elective, prompt | >90% with surgery |
| Medium | 250–400 μm | Prompt referral | 85–90% with surgery |
| Large | >400 μm | Urgent referral | 75–85% with surgery |
The minimum hole diameter (measured at the narrowest point on B-scan) is the key measurement. Also document:
- Base diameter: Measured at the level of the RPE — larger base means more complex surgery
- Hole form factor: A narrower, "pinched" hole has better spontaneous closure potential
- Subretinal fluid cuff: Hypo-reflective crescents at the hole edges — present in most full-thickness holes, helps confirm the diagnosis
- EZ and ELM disruption extent: Predicts visual prognosis after surgery
ERM vs. Lamellar Hole vs. Macular Pseudohole
Three entities that look similar on fundus exam are distinguished by OCT:
- Full-thickness macular hole: Complete break through all retinal layers; hypo-reflective defect from ILM to RPE; fluid cuffs at edges; treated surgically
- Lamellar macular hole: Partial-thickness defect, inner retinal loss with outer retina intact; usually ERM-related; managed conservatively unless symptomatic
- Macular pseudohole: ERM with central opening creates fundus appearance of hole; OCT shows intact retinal layers beneath the opening; no surgical urgency
Key Takeaways
- ERM staging (1–4) is OCT-based — B-scan determines surgical candidacy, not VA alone
- EZ band continuity is the single best predictor of post-operative visual outcome for ERM
- VMT footprint width <1500 μm has higher spontaneous resolution rate
- Macular holes: measure minimum diameter; refer promptly — outcomes degrade as holes enlarge
- OCT distinguishes full-thickness hole from lamellar hole and pseudohole — the fundus exam cannot
Educational illustration — ERM (violet line on ILM surface) and full-thickness macular hole with subretinal fluid cuffs (cyan). Real clinical scans in full course.
Sign up to track your progress and access all lessons.
Create Free Account